What an AI-Powered Staffing Engagement Looks Like
Pairing trained virtual staff with AI across intake, QA, coding, and back-office, what hybrid AI+staffing actually looks like in home health and hospice.
Lime Health Team
Lime Health AI

Most home health and hospice agencies eventually face the same problem: not enough trained people, too much manual work, and software that automates pieces of the workflow but leaves big gaps. The traditional fixes, outsource to a coding company, hire a virtual assistant, license another point-solution SaaS, each address one slice of the problem. None of them solve it.
There’s a better model emerging: AI software paired with a dedicated team member trained to operate it. Not AI replacing humans. Not humans without AI leverage. Both, working together, in your EMR.
This post walks through what that actually looks like, what the problem is, why neither AI nor staffing solves it alone, and what a real engagement at a home health or hospice agency feels like.
The Problem: AI Alone Isn’t Enough
AI is powerful. An ambient scribe captures a patient encounter and generates structured documentation in minutes. AI ICD-10 coding suggests accurate codes from clinical notes. AI OASIS QA flags inconsistencies in real time.
But every AI capability needs an operator. Someone has to:
- Review and approve AI-generated documentation before it syncs to the EMR
- Triage flagged issues, which need clinician follow-up, which are AI false positives
- Handle the work that falls outside the AI’s competency (complex cases, unusual diagnoses, nuanced compliance questions)
- Coordinate handoffs with the rest of the team (clinicians, supervisors, billers)
- Communicate with referral sources, payers, and patients
If you don’t have someone running the AI day-to-day, the AI’s value drops dramatically. Charts pile up unreviewed. Flagged issues go uninvestigated. The same operational drag that motivated the AI purchase reasserts itself, just with more software licenses.
This is why agencies that buy AI software-only sometimes report disappointing ROI. The AI works fine. The implementation gap is the missing operator.
The Other Problem: Staffing Alone Isn’t Enough
The mirror-image problem shows up with traditional virtual staffing or outsourced services. You hire a virtual coder, a virtual intake coordinator, or an outsourced billing service. The work gets done, but slowly, and at a cost that scales linearly with volume.
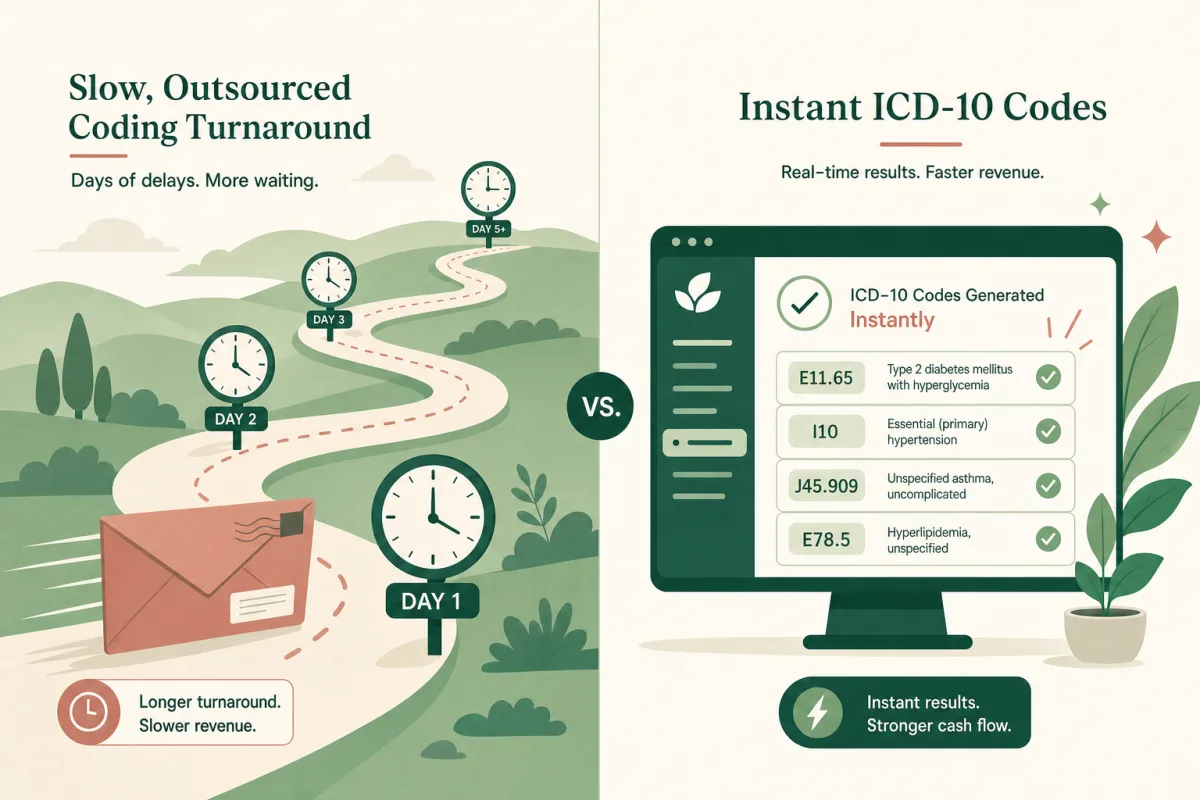
A traditional virtual coder reviewing charts manually takes 15-20 minutes per chart. An ICD-10 coder armed with an AI that drafts codes from documentation takes 3-5 minutes per chart. Same person, 4-5x output, same compliance posture.
Staffing without AI is a fixed-margin business. You pay for hours; you get hours of output. If volume doubles, costs double. If a coder leaves, you ramp a replacement for 4-6 weeks. There’s no leverage.
What an AI-Powered Staffing Engagement Actually Looks Like
Now imagine the bundle: a dedicated, trained virtual team member, plus the AI software that amplifies their work, deployed together at the same time.
Here’s what a typical engagement looks like across the five most common service categories:
Virtual ICD-10 Coding (Coder + AI)
Your virtual coder is a credentialed ICD-10 coder with home health and hospice experience (CCS, HCS-D, HCS-H). On day one of the engagement, they get access to your EMR and to the Lime AI ICD-10 coding platform.
When a chart is ready for coding, the AI drafts ICD-10 suggestions with clinical evidence mapping, pulling from the visit note, OASIS assessment, and supporting documentation. The coder reviews the draft, validates against clinical guidelines, applies coder judgment to ambiguous cases, and finalizes the codes.
Output: same-day or 24-hour coding turnaround at a predictable monthly cost, typically lower than per-chart outsourced coding, with higher PDGM accuracy because the AI captures comorbidities a generic coder might miss. See Virtual Coding Staff.
Virtual OASIS QA (Reviewer + AI)
Your QA reviewer is OASIS-E2 trained (often COS-C credentialed). Paired with Lime’s AI OASIS QA platform, they review every chart your agency produces, not just a sample.
The AI flags inconsistencies, missing M-items, scoring conflicts, and PDGM optimization opportunities in real time. The reviewer triages the flags: confirms real issues, dismisses false positives, and provides structured feedback to clinicians.
Output: 100% chart review (instead of 10-20% sampling), faster turnaround, and a clinician feedback loop that actually changes documentation behavior. See Virtual QA Staff.
Virtual Intake (Coordinator + AI)
Your virtual intake coordinator is trained on home health and hospice referral and admission workflows. The Lime AI intake automation platform parses incoming referral documents, verifies eligibility in real time, and pre-populates draft admission notes.
The coordinator handles routine referrals end-to-end (the AI does most of the heavy lifting), and escalates complex cases to your in-house team with all relevant data already gathered.
Output: referral processing time drops from 30-60 minutes per referral to under 10 minutes. Eligibility errors at admission drop dramatically (because the AI catches them before the coordinator does). Time-to-admission compresses from days to hours. See Virtual Intake Staff.
Virtual Back-Office (Coordinator + AI)
Your back-office team member handles scheduling, document management, payer communications, and admin. AI document parsing and workflow automation eliminates the highest-volume repetitive tasks (incoming fax processing, document filing, data entry between systems).
Output: clinicians and managers freed from operational work; consistent execution on the admin tasks that get dropped during volume surges. See Virtual Back-Office Staff.
How the Engagement Actually Works
A typical AI-powered staffing engagement at a home health or hospice agency follows this pattern:
-
Discovery: We learn your workflows, EMR, volume, and the specific gaps you’re trying to fill. We discuss whether the engagement includes the Lime AI platform (it often does, at no additional cost).
-
Match: We identify the right virtual team members from our trained roster, already familiar with WellSky, MatrixCare, HCHB, Axxess, DSL, and other post-acute EMRs.
-
Onboard: Your virtual team learns your specific policies and escalation paths. EMR access is provisioned with the same controls as your in-house staff. If AI software is included, it deploys alongside the staff onboarding, same go-live, same training cycle.
-
Integrate (Virtual staff work as part of your team) joining standups, using your communication tools, and reporting through your management structure. AI software accelerates both your virtual team and your in-house team.
-
Scale: Add or reduce capacity as volume changes. No long-term hiring commitments.
The whole process from discovery to live operation typically takes 4-6 weeks.
Why Lime Bundles Both
Most staffing companies provide labor. Most software companies provide software. Lime is the only post-acute service that bundles both, and we do it because we believe the AI delivers maximum value with a trained operator running it.
A trained operator turns AI capability into agency outcomes. Without that operator, AI becomes another underutilized SaaS license. With them, AI is the leverage that lets a single virtual team member handle the workload of 3-5 people working manually.
That’s why we often include the Lime AI platform at no additional cost in staffing engagements: the AI works best when paired with a trained team member, and the bundle is what actually moves the needle for your agency.
The Result: Staff That Operate at AI Speed
The combined model produces something neither pure AI nor pure staffing can deliver alone:
- Predictable cost, fixed monthly staffing cost, not per-chart pricing that scales linearly with volume
- Faster turnaround, same-day or 24-hour SLAs because AI does the heavy lifting and the operator validates
- Higher quality, clinical judgment from the human, consistency from the AI, dramatically fewer errors than either alone
- Better leverage on your in-house team, the same AI helps your existing staff, not just the virtual team
- No hiring overhead, no recruiting, no onboarding lift, no 4-6 week ramp-up if someone leaves
When Does This Make Sense?
AI-powered staffing is a fit if your agency:
- Has trouble hiring or retaining experienced post-acute talent
- Faces volume that fluctuates seasonally or unpredictably
- Has gaps in a specific function (OASIS QA, coding turnaround, intake) that bottleneck the rest of the operation
- Is growing faster than you can hire
- Currently uses outsourced services and wants higher quality at predictable cost
It’s not a fit if you have stable, fully-staffed operations and don’t need additional capacity. The economics work because we’re providing leverage; if you don’t need leverage, you’re better served by your existing team.
Related Reading
- Virtual Staffing Overview, All service categories with detailed descriptions
- Virtual Intake Staff, Referral processing and admissions
- Virtual QA Staff, OASIS-E2 and HOPE chart review
- Virtual Coding Staff, Certified ICD-10 coders for home health and hospice
- Virtual Back-Office Staff, Scheduling, document management, admin
- AI vs Outsourced Coding, Why AI-augmented coders outperform traditional outsourcing